
Aetos Transitional Care Management Services aid patients during transitions between healthcare settings, ensuring smooth shifts, improving outcomes, and reducing complications.
20%Readmission
Around 1 in 5 Medicare beneficiaries in the US experience hospital readmission within 30 days of discharge.
76%Readmission
A streamlined TCM program is projected to reduce readmission rates by up to 76%, consequently improving patient outcomes.

Understanding Transitional Care Management
Transitional Care Management (TCM) targets the post-discharge phase as patients move from a healthcare facility to their home or another environment. Its goal is to assist patients during this pivotal time, minimizing readmissions and complications, and enhancing health outcomes.
"Tailored care that adjusts to life's pace"
Core Capabilities

User-Friendliness
Facilitating seamless integration into current workflows with user-friendly features.
Engaging Communication
Initiating interactive patient contact within two days of discharge.

Post-Discharge Overview
Discussing the discharge summary and instructions with the patient or caregiver.

Smooth Care Transition
Collaborating with other healthcare professionals who will assume or continue care.
Knowledge Transition
Delivering seamless information transfer to the patient or caregiver.
Coordinated Care
Identifying patient needs through coordination with community organizations for care.
Medication Review
Delivering medication reconciliation.

Reminder for Follow-up
Automatically scheduling and reminding patients of necessary physician follow-ups or additional services.
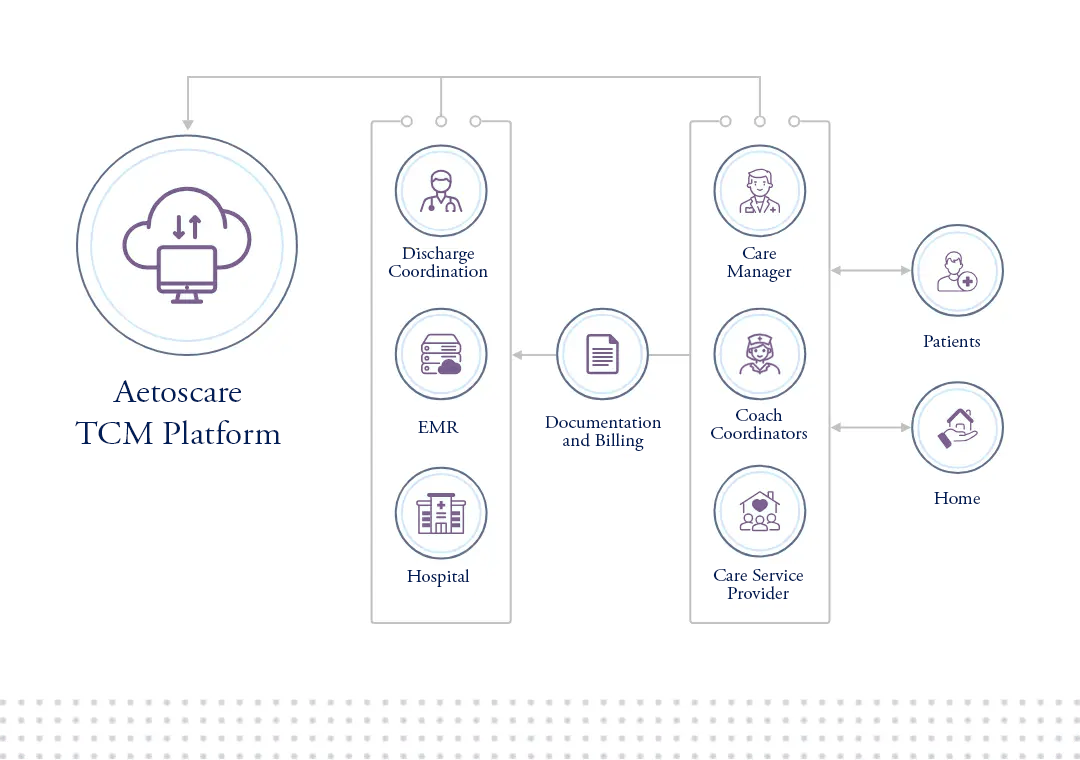
How it works
Our solutions facilitate scheduling face-to-face appointments, extending remote care, and accessing real-time patient health data through bi-directional EHR integration.
An interactive dashboard grants providers access to patient information and tools to efficiently deliver TCM activities.
During the transition from inpatient hospitalization to community care, TCM services typically encompass three categories.

Engaging Communication
This can occur through email, telephone, or face-to-face interaction within 2 business days after a patient's discharge to a community setting.

Remote Service
Gathering/reviewing discharge details, liaising with healthcare providers, offering education and support for scheduling follow-ups, treatment adherence, and medication oversight.
In-Person Appointments
In-person appointments can also be arranged, typically within 7 to 14 days, based on the complexity of medical decisions for discharged hospital patients.